
Cancer patients often ask their doctors, “What would you do if you were me?” Here, our Curious Dr. George asks Mayo Clinic oncologist Javier Munoz, MD, MS, MBA, how he would handle his own diagnosis of mantle cell lymphoma. At the Mayo Clinic in Arizona, Dr. Munoz serves as Director of the Lymphoma Program, Co-Director of the Cellular Therapy Program, and Director of the Cancer Center Clinical Trials Office.
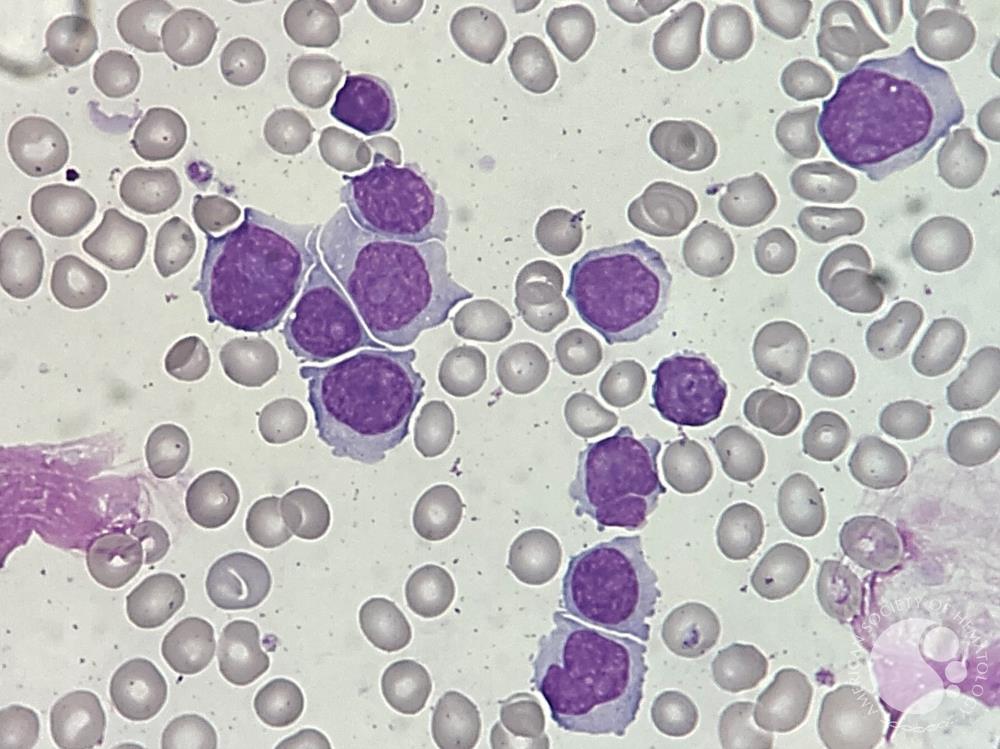
Curious Dr. George: Please consider this hypothetical scenario: You are a young male physician in general good health in an active practice of clinical oncology. You have recently experienced unintended weight loss of 15 pounds, loss of appetite, general malaise, and a low-grade fever with sweating at night. You consult your primary care physician who observes skin and mucous membrane pallor and palpable lymph nodes in your groin and axilla. She orders a complete blood count, which finds a hemoglobin of 11, a normal white blood cell count, mild thrombocytopenia, and relative lymphocytosis. Biopsy of an axillary lymph node results in the diagnosis of mantle cell lymphoma. How would you proceed?
Javier Munoz, MD, MS, MBA: Mantle cell lymphoma (MCL) is a rare disease with an ominous prognosis. If I were facing my own high-risk MCL, I would begin by acknowledging the shock. As oncologists, we often speak of probabilities and protocols, but when the disease becomes your own, those numbers carry a different weight. The first step would be to breathe, to process, and to gather the right team—a reminder that none of us, even physicians, should walk this path alone. High-risk disease may be defined by TP53 alterations, aggressive histological features like blastoid/pleomorphic morphology, or a high proliferation rate (e.g., Ki-67 index of 30% or greater). In this fictional case, my MCL is high-risk due to the presence of a TP53 mutation which historically heralds resistance to conventional chemotherapy agents.
After confirming pathology, morphology, and proliferation rate, I would seek enrollment in a clinical trial. MCL has long been considered incurable (outside of allogeneic stem cell transplantation), but that paradigm may soon be shifting with novel agents and cutting-edge clinical trials. The TRIANGLE and BOVen studies have introduced BTK inhibitors into the frontline management of this disease, suggesting that patients may avoid the toxicity of high-dose chemotherapy and autologous transplant. Knowing this, I would likely choose a chemo-free, novel-agent regimen rather than intensive chemotherapy for my own case of newly diagnosed TP53-mutated MCL. Outside of a clinical trial, I would choose for myself the triplet explored in the BOVen trial (zanubrutinib, obinutuzumab, and rituximab), which now appears in national cancer guidelines as an option for patients with TP53 mutations. Because of the TRIANGLE trial, I would personally shy away from accepting consolidation with autologous stem cell transplantation when achieving first complete remission in MCL.
I would continue to surround myself with positive, uplifting people and go through this journey day by day. If you have been diagnosed with cancer, there will be days that you will not know what the right way forward is. It is not a right or wrong situation, but rather what feels right to you. Find solace knowing that many have walked through this pathway before, and you do not have to walk alone. Regarding second or even third opinions, your doctor will never be upset, as we embrace collaboration and learning from you and our colleagues.
If my disease were to relapse, I would look toward CAR T-cell therapy, such as brexucabtagene autoleucel or lisocabtagene maraleucel—treatments that have yielded remarkable remissions for patients who once had no good options. CAR T-cells seem to be the great equalizers as they seem to work both for TP53-mutated and TP53 wild-type MCL. These therapies are not without risk—cytokine-release syndrome, infection, and neurologic side effects can be daunting—but I would be willing to endure the risks in exchange for the benefits of remission with a long-term horizon.
On a personal level, I imagine the greatest challenge would be relinquishing my instinct to analyze every data point and instead embracing the need to live fully in the moments between treatments. I would lean on my family, my colleagues, and my patients, whose courage has always reminded me that healing is as much about connection as it is about medicine.
For anyone newly diagnosed with MCL, my advice is simple: find a team you trust, seek second opinions, and ask about clinical trials. Revolutions in cancer care are built on hope—and in MCL, that revolution is happening right now with a quickly changing therapeutic paradigm. The future is indeed bright for MCL. By enrolling and believing in clinical trials, we can tailor such future together and ultimately cure MCL.
For publication questions, contact gdlundberg@gmail.com. For appointments with Dr. Munoz, contact ARZHEMONCNPS@mayo.edu.

.jpg)
.jpg)